
























![[Translate to English:]](/fileadmin/user_upload/images/menu/menu_service_downloads_broschueren.jpg "[Translate to English:]")








![[Translate to English:]](/fileadmin/_processed_/7/7/csm_menu_unternehmen_ueber-schell_awards_f6cec25b1d.jpg "[Translate to English:]")
![[Translate to English:]](/fileadmin/_processed_/a/0/csm_menu_unternehmen_ueber-schell_wasser-sparen_41036d2dd9.jpg "[Translate to English:]")





Hospital hotspots for drinking water hygiene: smart solutions for touch challenges – part 1
5-minute read
Where else, if not in hospitals, would you find the very highest requirements for hygiene? An effective hygiene plan needs to take account of many different aspects. Alongside hand hygiene, room hygiene and indoor air hygiene, drinking water hygiene at wash basins, showers and WCs is also very important. In this post, SCHELL’s resident drinking water expert Dr Peter Arens presents a number of challenges for drinking water hygiene in hospitals and the hygienic optimisation strategies used to meet them. Alongside explaining the corresponding standards, Arens also has several practical tips for HVAC and sanitation professionals, planners, building operators and other stakeholders. These strategies are naturally not just relevant for hospitals but can be usefully applied to many other buildings within the public sector. In part 1 of his two-part post, Arens introduces the following three challenges:
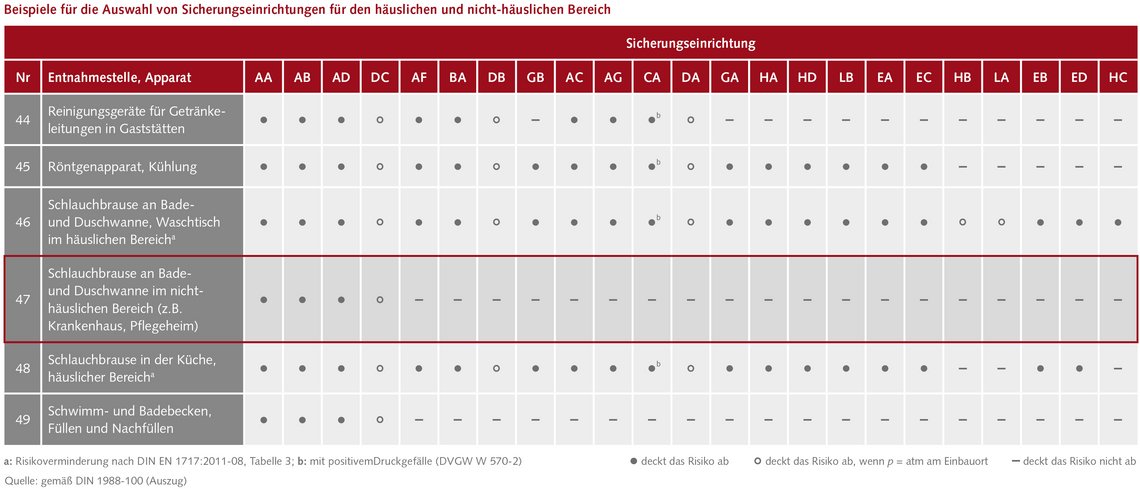
Challenge number 1: hand showers in non-domestic applications according to DIN 1988-100
“Although the terminology is a bit cumbersome, it’s talking about probably the biggest difference between this standard and practice within the HVAC and sanitation industry,” Arens reports. According to DIN 1988-100, table 1, row 47 (fig. 1), hand showers corrected directly to the drinking water installation are not envisaged for use in “non-domestic applications” – such as hospitals. These hand showers may be connected to the drinking water installation only via an air-gapped outlet (type AA, AB or AD) or a type DC pipe interrupter – i.e. only indirectly. “The authors drew up this rule because they were concerned a hand shower could end up under the maximum non-return height of shower or bath water during use or cleaning. If negative pressure then developed in the system, the contaminated shower/bath water (maximum category 5, as per DIN EN 1717) would be drawn into the drinking water installation via the hand shower. A simple backflow preventer would be of no use here – only one of the safety devices as mentioned above,” Arens notes. So is there an alternative system that can be used instead of these expensive safety devices? “Yes,” explains Arens.
Achieving safety objectives without safety devices
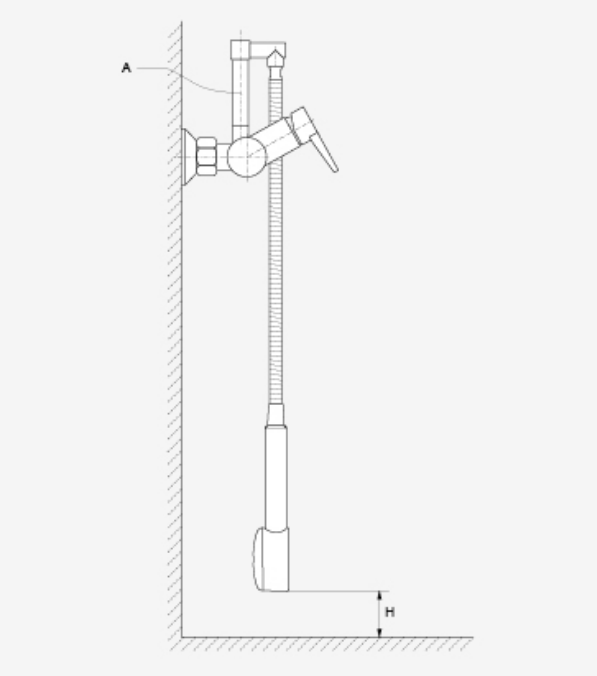
While still meeting all of the safety objectives in full, a simple remedy here is just to use a hand shower short enough to keep the shower head suspended at least 20 mm vertically above the maximum non-return height of the bathtub (fig. 2, letter ‘H’). In day-to-day operations, however, this can cause problems because nursing staff are unlikely to accept hoses so short that they are prevented from providing adequate care to patients. So another system is needed, to be able to still install the normal hose length of about 160 cm. To do so, this kind of shower hose is connected at least 162 cm above the bathtub’s maximum non-return height.
“For a concealed fitting, you would simply relocate the piping about 52 cm upwards (shower fitting height: 120 cm, shower tray non-return height: 10 cm) and then fit a flush-to-wall connection bracket for connecting the shower head hose. A similar approach would be used for an exposed fitting, also available with an upwards-angled outlet plus piping (cf. fig. 2, letter ‘A’) – like SCHELL’s VITUS series. Hand showers connected in this way would also remain compliant with the safety objectives set out in DIN EN 1717 and DIN 1988-100 in private-sector applications, without the need for expensive safety devices or a failure to uphold the safety objectives listed in the standards,” Arens explains. Connections using this approach also offer another advantage for day-to-day hospital life. Arens: “Shower heads connected in this way can no longer fall onto a patient’s feet while they are washing or being washed, which therefore avoids the risk of extremely painful mid-foot fractures.”
Challenge number 2: self-draining shower hoses
“This question has probably been being asked for the last 20 years or so and unfortunately answered wrongly just as often, although it has been definitively clarified by research from at least two hygiene institutes (Innsbruck and Gelsenkirchen) for the same amount of time and is also logical from a microbiological perspective,” Arens reports. “Bacteria under stress form biofilms more readily. These not only offer temporary protection against desiccation but are also known to give them an effective defence against disinfectants.” In experimental studies, shower hoses drained temporarily exhibited a significantly higher biofilm-associated bacterial load compared with water-filled shower hoses. In the study by the Innsbruck lab, this produced a significantly higher risk of infection. For hygienic reasons, the clear recommendation is therefore to avoid using any devices that provide self-draining functionality for shower hoses.
Challenge number 3: wash basins without an overflow or sealed siphon
In accordance with guidance from the RKI, wash basins in nursing facilities should be installed without an overflow. The water from the tap should also not flow directly into the siphon – which is not sealed. Arens explains the hygienic arguments for setting these rules: “Overflows are anathema to good hygiene: the dark sludge that coats them, consisting of fungi and microorganisms, can be seen easily with the naked eye although it is highly resistant to day-to-day cleaning efforts.” If no overflow is present, then the drain must not be sealable, to avoid the basin overflowing. This creates some hygienic challenges. “Because the drain is open, tap water must not be directed straight into it. This would dislodge bacteria from the siphon upwards and spray them onto the hands of users,” Arens explains. Research has shown that these bacteria can even enter the drinking water installation via the flow regulator in cases where reliable specified normal operation has not been secured. But the solution is often very simple. “The safety objective here is ‘Do not direct the water jet onto the open siphon’. So we need an inexpensive way of moving the jet contact point and this is often achieved simply by changing the flow regulator or (a bit more expensive) the outlet length (fig. 3).” Alongside flow regulators, SCHELL naturally offers wash basin taps with various outlet lengths, such as the wall-mounted VITUS series fittings series, and in different sizes, such as the XERIS E-T series.

Reusing optimisation strategies
The three examples illustrate the depth of analysis required for drinking water hygiene in hospitals. Yet they also offer valuable guidance, as Arens sums up: “The experience we gain in healthcare facilities gives us something like a highly magnified view of hygienic optimisation strategies, which can then be applied to other buildings in the public sector. The technologies required to do so are already available, as can be readily seen with the example of contactless fittings for wash basins and WCs.” Even in hospitals, less can sometimes be more. “The anecdote about self-draining hoses shows that, sometimes, it is better to avoid installing extra components to achieve good hygiene.”
Dr Arens introduces another set of challenges in part 2 of his post.
